Medicaid has a critically important role within the expansion of healthcare as spelled out in the Patient Protection and Affordable Care Act (PPACA). However, as a state run health program, Medicaid is often used as a political tool. It is important that those involved in and committed to changing healthcare be aware of the role Medicaid plays at the state level, and what we can do to help with healthcare innovation in our communities. Occupy healthcare will be examining Medicaid over the course of the next few weeks to help explain how this vehicle often drives state level healthcare policy, and how this vehicle is often highly susceptible to political influence. In this the first article of our series, we will examine the basic tenets of Medicaid and explain why this program is so important within our states.
To kick off this post, let’s start with a simple definition of Medicaid:
“Medicaid is the United States health program for certain people and families with low incomes and resources. It is a means-tested program that is jointly funded by the state and federal governments, and is managed by the states. People served by Medicaid are U.S. citizens or legal permanent residents, including low-income adults, their children, and people with certain disabilities. Poverty alone does not necessarily qualify someone for Medicaid. Medicaid is the largest source of funding for medical and health-related services for people with limited income in the United States.”
One point to make here has to do with the role the federal government has within Medicaid. You see, as states are responsible for Medicaid (what they do, how much they spend, etc.), federal government has what’s known as a “match” to help states run their Medicaid programs. From Wikipedia:
“Unlike Medicare, which is solely a federal program, Medicaid is a joint federal-state program. Each state operates its own Medicaid system, but this system must conform to federal guidelines in order for the state to receive matching funds and grants. The matching rate provided to states is determined using a federal matching formula (called Federal Medical Assistance Percentages), which generates payment rates that vary from state to state, depending on each state’s respective per capita income. The wealthiest states only receive a federal match of 50% while poorer states receive a larger match. Medicaid funding has become a major budgetary issue for many states over the last few years, with states, on average, spending 16.8% of state general funds on the program. If the federal match expenditure is also counted, the program, on average, takes up 22% of each state’s budget.”
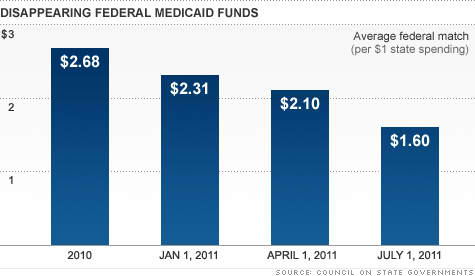
The problem with the federal match for Medicaid is that the amount of dollars the federal government is putting in to states is decreasing. “States regularly get matching funds from the federal government to help cover Medicaid burdens. But they’ve enjoyed an enhanced federal Medicaid match, thanks to the 2009 stimulus bill. The federal government sent an average of $2.68 for every dollar a state spends on Medicaid, up from $1.61 before the American Recovery & Reinvestment Act was passed, according to the Council of State Governments.”
As seen in the graph below, the decrease in these dollars subsequent to the drying up of enhanced federal dollars means that a heavier burden is placed on states to provide healthcare coverage through Medicaid. Think of the implications of this – if a state expands healthcare programs under enhanced federal dollars and then those federal dollars go away, the state is responsible for the new programming (and cost associated with that programming). However, it could possibly be the public using Medicaid who suffers when their new services go away because their respective state cannot afford them anymore (much more on this later in the series). And think about the top two “line items” that are often cut at the state level – yup, you guessed it – healthcare and education.
No question, expanding health insurance coverage to those who are uninsured or under insured is an essential component of PPACA. There is a logic behind this expansion that asserts when we offer affordable coverage to individuals and families that have no coverage, they are more likely to use healthcare services appropriately rather than waiting on someone to get really sick and showing up in the emergency department at their local hospital. We know that “uncompensated care” can be a significant driver of healthcare cost (see other OH posts on the costs associated with healthcare and how this remains one of our most significant barriers to overcome in any health reform effort). Theoretically coverage should open the door for individuals to receive more preventative services (helping keep people healthy) and less acute care services (often very costly).
According to 2009 numbers, there are almost 52,000,000 individuals enrolled in Medicaid (this includes children through the Children’s Health Insurance Program – CHIP). These are significant numbers when one considers that the last census data shows there are over 307,000,000 people in the United States. And it is clear that while Medicaid is not only important to the millions who depend on it for their healthcare, it is also important to those not being covered by it.
A recent Kaiser Family Foundation Poll found that 39% of those surveyed believe Medicaid was very important to them and their family. As seen below, Medicaid is a pretty important program for our country. In this same poll, the authors provide some context for why these data are important in our national dialogue on healthcare.
“If you listen to the inside debate you would think Medicaid is America’s most unpopular program. Conservatives don’t like Medicaid on ideological grounds; it’s a government entitlement program. Providers complain about the program’s reimbursement rates. And liberals have long complained about the program’s limitations, especially the gaps in whom Medicaid covers and the large variations in coverage among states. With its joint federal-state financing and welfare-linked heritage, Medicaid is treated as fundamentally different than the two other big entitlement programs — Social Security and Medicare — and thought to have dramatically less public support.”
Thus, politics begins to enter into the equation. In our next post on Medicaid, we will discuss how Medicaid is often used for political gain and how this sometimes works in the favor of those looking to innovate, but often works against those receiving Medicaid services.
For more information on Medicaid, I highly encourage you to peruse the Kaiser Family Foundation’s Primer on Medicaid. In this article there is a significant amount of general information on the program and what role Medicaid plays in local, state and national healthcare.