It is impossible to get away from conversations on healthcare without talking about money. There is good reason for this. Unless we start to understand the “economic engine” of healthcare, it is hard to make an argument about what needs to change.
And make no mistake, something is going to have to change.
From Reuters:
“In its annual budget and economic outlook, the non-partisan Congressional Budget Office said that even under its most conservative projections, healthcare spending would rise by 8 percent a year from 2012 to 2022, mainly as a result of an aging U.S. population and rising treatment costs. It will continue to be a key driver of the U.S. budget deficit.”
Healthcare is expensive, and growing more expensive by the day.
Yes, we can talk about changes in clinical delivery and the like, but really clinical services are often driven by payment for those services. The healthcare system has been built around expensive services (volume is important to discuss here, but we simply spend more on services period) – this is nothing new, but are there possible explanations we can offer for this?
Increase in high cost technology and rise in prescription drugs cost?
Increase in chronic disease and people living longer?
These are all likely contributors to the problem, but really isolating one will not likely lead to a solution. Hence the tie in with the Money Pit.
For those who do not remember, the Money Pit, starring Tom Hanks is a comedy about a family who gets a “deal” on a house only to find out that they will need to put a lot of money into the house just to make it liveable. The good deal quickly becomes a big problem. When one problem is highlighted and fixed, another problem rears its ugly head. No matter how many “fixes” there are on certain problems it is the entire house that is really falling apart.
Healthcare is really much of the same way. We can throw money and good ideas at part of the problem, but if the house is fundamentally “unfix-able” what do we do? Can we simply replace on e part of healthcare and hope it has an impact on other aspects of healthcare? Maybe in some cases it will, but it appears that determining a priority to address in healthcare may be more challenging (because there are so many moving targets).
I like to call this the “band-aid on top of a band-aid” phenomenon. So where do we start? Well, where are we spending the most money?
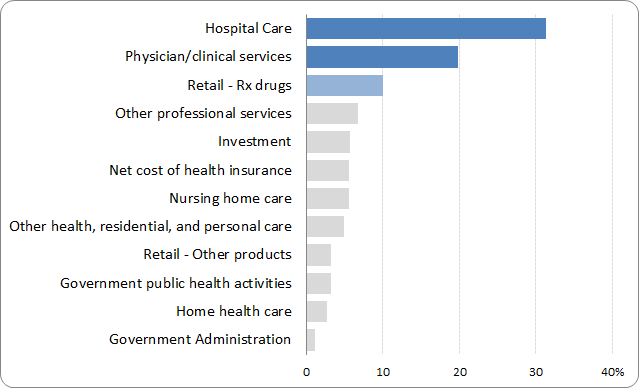
The graph below shows, we spend a lot of our healthcare dollars on and in hospitals.**
From an interview with ABC news, Gail Wilensky stated: “We have a system that encourages more and more complex services to be provided, whether or not that is necessarily the best or most appropriate care, partly because of how we reimburse our physicians in the hospital”.
I think we can all agree on the need for new business models in hospitals. But really, this is bigger than hospitals.
I do not need to go back into some of the same topics I have written about before on this topic, but I do think we should continually be thinking of what role healthcare costs play in any and all health reform efforts.
These issues will not be going away any time soon. Just like Tom Hanks, we are stuck in a “money pit” and it is just a matter of time before we realize it.
**Many thanks to David Napoli (@biff_bruise) for making the above pie chart (apparently an aberration for statisticians) into the better, easier to read version below.
 About Ben Miller
About Ben Miller
 About Ben Miller
About Ben MillerDr. Miller has his doctorate in clinical psychology and is an Assistant Professor in the Department of Family Medicine at the University of Colorado Denver School of Medicine where he is the Director of the Office of Integrated Healthcare Research and Policy. His core task is to integrate mental health across all three of the department’s core mission areas: clinical, education, and research. Opinions expressed here are his own and not those of his employer.